Public Health and Infectious Diseases
in Southern Africa
Spring Semester 2016

In the spring of 2016, I enrolled in my first Honors Seminar through the University of Cincinnati. This seminar was taught by Dr. Jason Blackard, who I had known previously as the faculty advisor for GlobeMed, and was an introductory course to public health, with a specific focus on HIV/AIDS, Tuberculosis, and Malaria, in Southern Africa. During the course of the semester, the small class of 11 students and two faculty members discussed, in particular, public health in the southern African nations of Botswana and South African. Discussions focused on topics related to the culture, history, demography, disease prevalence, and public health infrastructure of these nations, and was very informative and insightful. With a comprehensive exploration of HIV in particular, both the biological and social /population-level underpinnings of the disease were covered. This -- along with the interdisciplinary nature of the course -- provided a great framework to understanding public health from multiple different avenues.
|
Over the course of the semester, in addition to in classroom discussion, guest lecturers, textbook readings, and supplemental instructive materials, the students in our class completed regular assignments. The first of these, at left, is focused on the Millenium Development Goals and their successor -- the Sustainable Development Goals -- in South Africa and Botswana. Both of these southern African nations, like the rest of the world, have and are continuing to work to meet these United Nations international goals for development.
As we quickly learned, though, the success with which the two countries have actually met these goals has been very different. While Botswana's fairly small population size and relative wealth has seen its star rise on the international stage, South Africa has lagged behind its neighbor to the north. Contending with increasingly limited foreign aid as a result of heightened economic prowess, South Africa has not been as successful in developing at par. This distinction between the two countries is an important one to realize early on, and thus this assignment helped set the framework for the rest of the course.
|
|
|
|
Our discussion of HIV/AIDS in the classroom was also augmented by a discussion of the epidemic that the HIV virus created in the 1970s and 1980s. With a screening of the the film "And the Band Played On", we were able to learn more about the history of HIV/AIDS in our own country, as well as the social stigma that existed and still exists around the disease. The second class assignment was to write a short review of this very eye-opening film, which chronicles the history of the disease from governmental, social, and research-based lenses to give a holistic picture of the disease's evolution.
|
To further the dialogue on public health, our class also examined the role that ethics plays in public --and specifically global -- health. We were fortunate to learn from Dr. Anand Selvam, who is an emergency medicine physician and has extensive experience in public health. Dr. Selvam shared with his experiences in global health, but also the challenges that he has come to face as a result of his experience abroad. Students in our class were then asked to confront some potential ethical dilemmas of our own in our third class assignment.
|
Case 1: You are in a rural South African hospital. A prolonged government strike leads to severe staffing and resource shortage. There are no disposable gloves and many procedures are performed bare-handed. One day during rounds in the Labor Ward, the Chair of the department asks you to draw blood from an HIV-positive woman in labor as the team is presenting the patient in her room. The only remaining gloves in the hospital are a few pairs of sterile gloves reserved for emergency cesarean deliveries.
This situation is an interesting one in that it presents a number of different, interrelated ethical dilemmas. One the one hand, it is important to address the needs of the patient in question. Given the fact that the patient is HIV-positive and in the Labor Ward, her condition should be monitored closely, and if the medical team thinks that a blood draw is crucial to this monitoring, then the patient’s blood should be drawn to give her the best possible care. On the other hand, a blood draw for this HIV-positive patient also presents many concerns to others. To perform the procedure bare-handed would present a direct risk to my own personal safety, which would not only be something with which I would not be comfortable, but would also jeopardize the possible care of other patients. Given that the government health workers are on strike and staffing is limited, it is important that all caregivers and medical personnel that are available to keep patients healthy are available to do so. If I performed this procedure and contracted an illness, I would rationally want to return to the United States and seek medical treatment, which would leave the clinic in South Africa with one less worker and a harder time caring for its patients. Using a utilitarian understanding of justice, this would mean that performing a bare-handed blood draw for this patient would not be ethically right, given its potential harm to a large number of patients for the benefit of only one. Even if I opt to use one of a few remaining pairs of gloves in the hospital, this would not eliminate the existence of an ethical dilemma. To use the gloves for this simple procedure would be to jeopardize the success of Cesarean deliveries, which are arguably more important—especially in light of the possible years of life lost if a newborn contracted an illness and died because of a lack of sterility during birth. Moreover, while the clinic does not have disposable gloves now, these gloves are a lot cheaper than their sterile counterparts. Thus, if I used the more costly gloves for a procedure that did not warrant them, I would be wasting clinic funds that could be used in the future to ensure more optimal care for a large number of patients. In this way, using the gloves would also present a significant utilitarian concern. Not only does using sterile gloves jeopardize the life of a newborn baby born through Cesarean delivery, but it also has a future impact on clinic operations. Therefore, whether gloves are used or not, the “greater good” takes precedence over the needs of the individual patient in question, thus pushing me to refuse to perform the procedure altogether. This decision, in turn, does have the potential to alienate me from the medical team that is graciously hosting me, especially when considering that many on this team have already been exposed to HIV. Even so, I think that the consideration of the many other patients in the hospital takes precedence over my own comfort with the medical staff. In this case, avoiding a situation that is ethically questionable regardless of the action taken is more important than fostering good relationships with the medical team of the hospital. |
Case 2: You are a 1st year medical student in a rural South African HIV/AIDS clinic: It is your first day and there are twelve lumbar punctures that need to be completed after rounds. You are tasked with performing a lumbar puncture (LP) on a dying patient in an open air TB ward. You have never done one before and have only seen it performed once previously. A senior medical student is supervising.
I think that this situation is potentially the most challenging one that we discussed in class. Initially, my position was that I would not perform the lumbar puncture because I was not qualified to do so. As an aspiring physician, I know that it is my duty to ‘do no harm’, and I believe that were I to perform an LP without proper supervision from at least a resident—if not a fellow or attending physician—that I would be endangering this principle due to my lack of experience with the procedure. I was of the belief that when presented with this situation in real life, the only way that I would perform the procedure would be if it was to act as a team player, and get on the good side of the medical staff. From a Kantian perspective, this would be unethical, as my motivation for the action that I would perform would be tainted with a desire for self-advancement as opposed to patient care. Thus, in the classroom, I was staunchly opposed to performing the procedure. 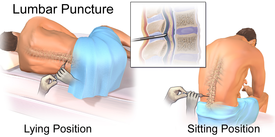
Given the information that I now know with regard to the ubiquity of medical students performing procedures in South Africa, my former position comes slightly into question. My initial concern that my lack of qualification would mean that I might endanger the patient’s safety is less concerning when considering that if I did not perform the LP, another medical student would. With this in mind, it would be very hard to ensure that the patient’s health is not endangered, as no matter my course of action, someone that I view as under-qualified to perform the LP will do so. In this way, I might even be able to minimize possible harm to the patient if I perform the procedure and take extreme care and caution when doing so—something which another medical student who would fill my stead were I to refuse might not do. When this thought is paired with another that I had not considered—the act of imposing Western views on a system of care that is the standard in South Africa—it becomes apparent that performing the lumbar puncture might not be so unethical an act at all. If anything, doing so would be ethically right if I was able to shift my motivations to focus more on the patient’s care and less on my own personal advancement. Even with this change that would qualify my actions as ethical from the Kantian perspective, the decision is still a difficult one when the utilitarian understanding of morality is considered. Even if my heart is in the right place when performing the LP for this patient, and even given the standard of care that exists in South Africa, at the end of the day, potentially exposing the other vulnerable patients in an open-air TB ward to any further complications from illness simply to take a lumbar puncture from a dying patient would not benefit the greatest number of people. Thus, I think that I would stay with my initial position on the issue, with the qualification that I could now totally understand taking the opposite course of action.
|
|
Perhaps one of the most interesting parts of the course was hearing about the human experiences attached to the HIV/AIDS epidemic in Southern Africa. As with any disease, HIV/AIDS is not just a matter of statistics, biology, and research. Rather, real people are affected by the illness, and their stories -- in my mind -- are important ones to hear. Some of those stories were shared in a novel that we read during the course of the semester, Saturday is for Funerals. This book highlights the stories of individuals while explaining medical background to their conditions. In doing so, it presents a very readable and informative depiction of the change in psyche that has come about as a result of HIV/AIDS in the places that it is most prevalent. In a sense, the novel gave great insight into life within the communities that are hardest hit by the virus. Our fourth assignment for the course was to review the book and its impact, as well as to prepare a list of questions for its author.
|
|
For our fifth class assignment, we broke the HIV/AIDS mold in which we had been set for the majority of the course, and explored a different disease in the region of Southern Africa. Though malaria is not nearly as devastating to populations in this part of the world as its HIV/AIDS and TB counterparts, it is still an important disease to discuss because of its prevalence. To give a holistic, broad-lens look at Malaria, the students in our class combined our research on the disease into a collective presentation that addressed it from multiple angles. Discussing everything from epidemiology and diagnosis to treatment and vaccines, the presentation was a collective effort to be proud. When presented, it helped put into greater context the extent of the challenges faced by public health professionals in this region.
|
|
|
|
The final project that we completed at the end of the course was an independent report that investigated a topic of interest pertinent to public health in Southern Africa. This project allowed students to integrate all that they had learned during the course of the semester, and to further explore a related area of intrigue.
My focus for this capstone project was traditional medicine in South Africa. From brief mentions in some of the texts that we read during the semester, I gleaned that traditional medicine still plays a big role in South African culture, so I sought to further explore this field. Upon further investigation, the idea that traditional medicine "still plays a role" is a major understatement. In fact, traditional medicine is the primary form of medicine for most South Africans. |
